.svg)



July 23, 2026

ERAS teams hustle to improve patient outcomes, save staff time, and optimize the patient experience.
But, due to staff shortages and overwhelmed providers, these teams still face challenges to get the most out of their ERAS initiatives:
- Patient education is manual and inconsistent across physicians, departments, and hospitals which is time consuming and leads to inconsistent patient outcomes.
- Clinical teams have no efficient way to ensure care plans are being followed so they can’t intervene and catch problems before it’s too late
- PROMs engagement is low and data collection is manual meaning clinical teams lose visibility on what’s working
For most, it’s because they haven’t invested in a way to standardize their ERAS programs across their health system.
During our recent Product Talk, SeamlessMD CEO, Dr. Joshua Liu, demonstrated how Digital Care Journeys can scale ERAS efforts pre- and post- surgery to empower patients beyond the hospital setting.
Following a live demo of the SeamlessMD platform, Dr. Liu shared clinically-validated data from a variety of different surgical departments and health systems who have seen marked improvements to their patient outcomes after implementing Digital Care Journeys.
“Patients get seamless on their phone, their tablet or computer, and they're guided pre and post care through a journey like enhanced recovery. And on top of educating patients along the way, they can track data and all the data that the patients track about their progress goes back to dashboards, alerts, and analytics so that your team has oversight on individual patient progress.” - Dr. Joshua Liu
What are the top 6 questions clinical ERAS leaders ask us?
1. I am interested in updates to pathways. For example, when our hospital began ERAS years ago, insulin infusions were recommended, but recent literature does not support this. Do your pathways evolve?
Dr. Liu: The SeamlessMD out-of-the box pre-built care pathways are designed and maintained by our clinical team. We call them patient education specialists. That team not only develops the pathways based on the latest evidence but typically at least once a year, they are reviewing those pathways internally and, and making updates to our templates.
All that being said though, what we don't do is make updates to your version of the pathway on SeamlessMD unless you've signed off on any changes. So what our team does is we may make recommendations to your teams based on what we're seeing, a change in practice, either in the evidence or from some of our key ERAS partners, and then let you decide if you want to make similar updates.
So you're always in full control of the content and pathways. But we certainly invest in keeping you updated and, and doing the research on our end as well.
2. Is there a physician interface? How does the hospital see the results from the app?
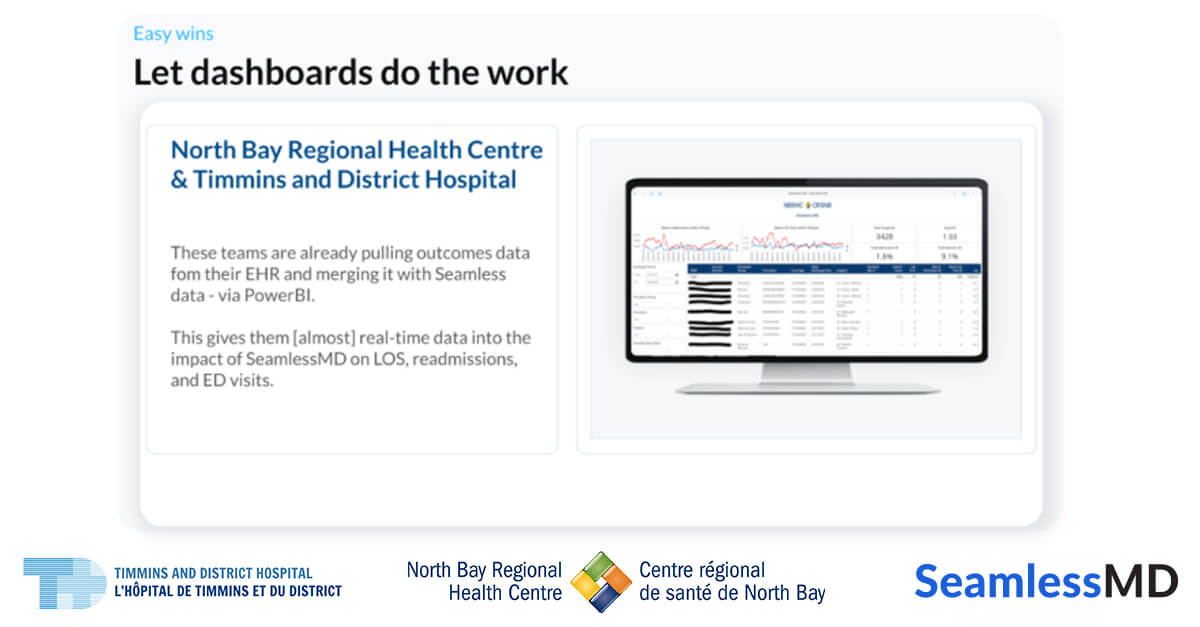
Dr. Liu: On the backend you can optionally get access to dashboards [the image below] for remote monitoring or more data and aggregate.
A lot of clinical folks using SeamlessMD, including physicians, nurses, and others will log into our backend portal to look at this data. And if it's integrated with your EHR, these dashboards actually show right up inside Epic, Cerner, or MEDITECH. So with an integration, we can even streamline the access to the data.


3. Is there an online-only option (is there a way for patients to access all of this information from their internet browser on a computer), or is it only for phones/ tablets?
Dr. Liu: Yes you can access it purely through your internet browser.
In fact, we have some patients who even if they have a smartphone or a tablet, they are using our browser. That's been really important because early on when we would sit next to patients and watch them interact with the platform, we noticed there were some elderly patients who didn't know their Apple App store password.But they could go into their browser and they could check their email. So being on the browser has been actually very important for patients, even if they have a smartphone or tablet.
4. Do you have any data or proof that an older patient population is using the app? How responsive are they to using the app?
Dr. Liu: Adoption for Seamless typically ranges from 60 to 70% all the way up to the high 90% range, depending on the demographic and how closely our partners follow our best practices for adoption.
One of the nice things about SeamlessMD is that early on our first partners were using SeamlessMD for frail elderly patients with complex surgical journeys. So we had to design from the ground up with this population in mind.
UAB actually presented data at the Academic Surgical Congress where across an almost 1,700 patient population in major cardiac, thoracic, colorectal and gynecology oncology patients, they saw a 94.7% patient adoption despite the average age being in the sixties for that population and it's a lower socioeconomic status neighborhood in Alabama. I think that's largely because not only have we followed all those accessibility guidelines and made it multi-platform, but UAB also did a great job in leveraging our best practices for adoption. We don't just hand our customers the technology and say, “I hope your patients adopt it”, we have a very close tight-knit partnership to drive adoption and success with clinical teams.
5. Can patients provide access to their Digital Care Journey to a family member or an at home care provider?
Dr. Liu: Yes, absolutely. The nice thing about SeamlessMD is that even though the patient is the core user, loved ones and family members can also enroll with the patient. We have some patients where it's one or it could be three or four caregivers with them in the journey. About half our patients actually choose to enroll loved ones with them to help keep them on track.
6. As the patient engages with their care pathway, does the health system need to "script" if the patient asks this or does SeamlessMD use AI?
Dr. Liu: Yes. On the patient side, it may feel like there's some advanced AI, but actually we use what we call more of an expert rule system. Wwe have a number of pre-built protocols and logic branching that's signed off and configured with your care team. So that way based on a certain path the patient goes down, the system automatically changes the patient journey dynamically.
For example, if we know that a patient is diabetic, either because we pull that from the EHR or because the patient self-reports that they are. Then those patients may get extra diabetes related protocols, questions and surveys. If they're not diabetic, they wouldn't get that. So there is a lot of pre-built intelligence, parameters, and branching to make it as tailored to each patient as possible.
Want to learn more about how to improve your ERAS outcomes with Digital Care Journeys? Watch the recording of our Product Talk featuring a live demo now.




.png)
