.svg)



July 23, 2026
Recovery after surgery is a complex process and different outcomes are important at different phases of the journey, both for patients and providers. Since Enhanced Recovery After Surgery (ERAS) was established as a practice, and as it increasingly becomes the standard of care, metrics that need to be measured for quantifying and setting the standards of the recovery trajectory continue to evolve.
ERAS protocols are leveraged by leading healthcare organizations in order to streamline a patient’s surgical journey – from pre-op preparation through post-surgical recovery – to reduce the patient’s surgical stress response and complications, improve the patient experience, as well as enhance clinical outcomes. The care pathways form an integrated continuum, as the patient moves from home through the pre-hospital / pre admission, preoperative, intraoperative, and postoperative phases of surgery and home again.
The ERAS® Society, for instance, has set in place several pre-, intra-, and postoperative protocols of surgery, alongside metrics such as rate of return, length of stay, direct cost, and complications that they recommend health systems measure in their ERAS programs, whether in one service line or across multiple pathways. In a 2021 study, the success of the institutional ERAS program was rated as 6.9 ± 2/10 while improving both patient outcomes (90%) and satisfaction (69%) were rated as main motivators for ERAS implementation.
With the numerous protocols to follow, identifying which data or metrics to collect, and analyzing them, is critical for the success of an ERAS program. As Dr. Kevin Elias, President of the ERAS USA Society and Gynecology ERAS Leader at Brigham & Women's Hospitals, says, “I do think it's important to have that data, at least a few of those core elements that you really want to impact. And pretty frequently, rather than quarterly or yearly because that's not often enough if you're trying to be reactive to staying on the protocol.”
Here’s a look at some of the metrics that leading organizations with multiple ERAS pathways measure, and scale, for consistent data collection.
ERAS Outcomes and Data Points to Measure
To meet the needs of individual patients and monitor clinical outcomes, ERAS teams need to be mindful of data integrity and collecting the right data, sharing it, and analyzing it. Ongoing data assessment can help determine whether the new protocols did indeed improve outcomes or if any changes that need to be introduced to ensure ERAS protocol compliance and consequent patient outcomes.
Charlette Hart, Director Surgery Administration at Baylor Scott & White Health, emphasizes that ultimately it is critical for the health system to understand why the data is being collected in the first place – “Are we collecting something just to be collecting it or are we collecting it because it's actionable and we're finding conclusions with that data that's helping us to improve? If we're finding that we're just collecting something to collect it, we stop collecting it. It needs to be something that we're able to use to improve our care.”
Common metrics to measure
At University Hospitals (UH), they focus on six patient outcomes - length of stay, readmission rate, mortality, surgical site infection, narcotic utilization, and variable cost. According to Dr. Heather McFarland, Vice Chair Operations and Director at Anesthesia Value Network, University Hospitals, these are outcomes “that senior leadership really looks at, but then more so outcomes that really drive our clinicians as well. So those are the six biggest things that we look at at this point.”
Measuring these outcomes go a long way in enabling organizational buy-in from leadership stakeholders as well. As Dr. McFarland notes, UH was able to decrease their LOS by 50% and “when you're dealing with a hospital capacity that is probably reduced secondary to a nursing shortage, you are able to move those patients through more quickly, which is very clinician driven and I think satisfying to them … When you talk about decreasing the length of stay by 50%, you're almost increasing your capacity by 50% because that can be filled again. Those two things have caught our senior leadership's attention in the time that we've been working on it.”
Granular metrics to measure
For Brigham, Dr. Elias shares, there are “different levels of data collection. We've participated in the ERAS Interactive Audit System, which is sort of an international registry for tracking ERAS outcomes, which tracks a lot of data at a very granular level. Looking at 70 elements per case. It's quite a lot. From a more practical perspective, for most of the service lines, we're looking at about 18 different items that are high-priority items of the ERAS Society.”
On a week by week basis, this means looking at quite a few process metrics for Brigham. Dr. Elias shares that he looks at “carbohydrate loading, opioid-sparing analgesic use, total opioids administered intraoperatively in the first 24 and 48 hours. And then looking at time to mobilization, time to advancement of diet, total length of stay, and major complications that have happened during the stay. For us, it's sort of a PDSA [Plan-Do-Study-Act] cycle. We're constantly looking to see our patients getting up and mobilizing in relatively short order, are we seeing good use of opioid-sparing techniques and very few outliers on opioid consumption.”
And having that data ready and analyzed as close to real-time as possible is key for making sure the ERAS program is on track and helps understand what process improvements are required in the pathway. “For us, our median length of stay for major site reductive surgery is three days. And the range is pretty tight. It's two to four days for 95% of patients. So when I started seeing a lot of patients that are creeping up in the five, six-day range, I started asking questions as far as where the program is broken down? And similarly, I started seeing patients with escalating opioid requirements. I'm looking at, what are they getting intraoperatively? What are we writing for? Why are we seeing so many outliers? Much like they saw at University Hospitals, our prescribing went down by about 75%-80% as far as OMEs that patients are going home with. So if those are ticking back up, then the question becomes, did something change in our operative management or is this an education issue to the prescribers?” shares Dr. Elias.
Increase in number of metrics measured as pathways are scaled
For Novant Health, the number of data points they measure for has changed as the ERAS program scaled across multiple pathways. Vicki Morton, Director of Clinical & Quality Outcomes for Providence Anesthesiology Associates and ERAS Program Leader at Novant Health explains they started with 20 data points in 2016, which has grown to “over 150 data points or something like that now. We always focus on the most basic patient outcomes that everybody does - readmission rates, length of stay, complications, all that. We look at postoperative nausea and vomiting (PONV), pain scores, opioid consumption. We look at probably a lot of things that maybe people wouldn't necessarily look at. But with every service line, it's part of our discussion – ‘Okay, what are we trying to fix? What data points around this are we looking at?’ And again, we have the core ones. But then anything in addition to that, we ask what do we need? … Through the years, we'll get some data requests such as ‘Maybe this isn't a data point that we're normally collecting, but let's talk about it. Maybe we should be collecting those with all services.’ It's grown. Then there are the compliance data points as well. So, you can look at your outcome data, but you also have to be measuring your compliance data. So if something's going awry within your outcomes, is it your pathway that needs to be changed or is it a compliance issue? You have to be able to distinguish between those two.”
Identifying ERAS Patients in an EMR/EHR
Data available through electronic medical records (EMRs) and in electronic health records (EHRs) provide further insight on how an ERAS program is implemented in an organization as well as analyze the impact of the program on surgical outcomes. However, even though identifying which patients are ERAS cases in an EMR/EHR is critical, it is not an easy task.
Implementing banner function
At Brighman, there are a few ways for them to decipher how a patient is part of an ERAS pathway. Dr. Elias shares that they “did implement a banner function so that it shows up at the top patient's chart when a patient is enrolled on an ERAS pathway. So at first, that was really important when you had some service lines that were using ERAS and some service lines which weren't – so that the nurses understood that they were being expected to rapidly advance patients. People always say, ‘What's a non-ERAS patient? Isn't everything an ERAS patient?’ Yes and no. I mean, if you have a patient who's been, let's say, readmitted with a re-op and is now in the ICU, that's hard to keep them on the ERAS pathway. So, it's important that you don't want a bunch of triggers that come from your order set for nurses to do things that maybe aren't actually aligned with best patient care. It's not that patients aren't being implemented by ERAS, but it's just that it might not be as much of a default checklist. And it's a little bit more selective choosing by their provider.”
Surgical reservation form field
For UH, the surgical department enrolls their patient in ERAS and the designation of whether a patient is on an ERAS pathway comes from the surgical reservation form field – ‘ERAS patient’: ‘yes’ or ‘no’. Dr. McFarland echoes Dr. Elias’ point that “it's much easier to collect data that is a designated entity of itself. And so, we work on the same thing. Every surgical patient gets a surgical update prior to going into the operating room. We actually have carb loading on that, and a ‘yes’ or ‘no’. Anytime you can modify your EHR, your electronic data gathering system to really become a distinct entity, it's extremely helpful for gathering that [data].”
Role of an EHR and Integrated Digital Tools in Consistent ERAS Data Collection
The role that EMRs and EHRs can play in identifying a patient’s ERAS or non-ERAS journey and efficient data collection, a robust, user-centric record system, as well as tools and processes that can supplement it, is key; and Dr. McFarland cautions of the challenges that come in its absence.
She shares “their ability to manage, collect, and look at outcomes – that has probably been our biggest struggle … We are focused on 20 core things that our clinicians can do to really improve what's happening in ERAS. We're hoping as we work with technology more, that we can begin to track those and find out really where we can dig in and do better for our patients. But at this time, it's those overall patient outcomes that we are looking at.”
Dr. Elias echoes this sentiment of having a robust EHR and identifying any modifications of supplementary tools required, suggesting that “As far as the EHR goes, one of the really important things is if there is metrics that you're having trouble collecting, then you want to have a discussion about how do we modify the EHR to make that happen? For us, a classic one was carbohydrate loading. How are we going to measure carbohydrate loading? Is it going to be a note the provider writes in the chart? Is it going to be a paper thing that they're going to write on the chart? Is it going to be an update? … Ultimately, we just created an element on the flow sheet so when the patients were in pre-op, in the PACU when the nurses were doing their intake, they asked them about the carbohydrate load. There were a couple of boxes and they just checked the one that applied to the patient. Now, all of a sudden you have a default field that you can abstract with a report. I think for high-value items like that, it's quite helpful. Same thing with our nursing flow sheet for post-op. We added an ERAS field where we could keep track of caloric intake and mobilization … Creating an element is really what you want to do for these big items.”
Health systems implement ERAS protocols with an aim to adhere to as many elements of the guidelines as possible to achieve the best possible outcomes, and manually optimizing and scaling ERAS programs across service lines poses additional challenges. This includes arduous data collection, such as manually collecting patient-reported outcomes (PROs) that require additional resources or ensuring patients adhere to protocols, which is often hindered by paper-based education and documents that could be lost or misplaced by patients.
Digital patient engagement tools, such as Digital Care Journeys that offer turnkey integrations into EHRs, can help tackle some of these challenges. Digital Care Journeys enable providers to deliver automated patient self-management ERAS education; send reminders to keep patients on track; remotely monitor patient health status, including patient self-reported pain levels, movement, opioid use, wound images, etc.; and measure patient compliance and adherence with ERAS protocols.
Digital tools integrated into an EHR also help automate the collection of patient-reported outcomes (PROs) for research and quality improvement. In fact, according to a study published in Science Direct, 81% of respondents (from surgical and non-surgical departments) indicated that the use of Patient-Reported Outcome Measures (PROMs) is or would be facilitated if they are integrated into the EHR.
Managing and Analyzing ERAS Data Across Multiple Pathways
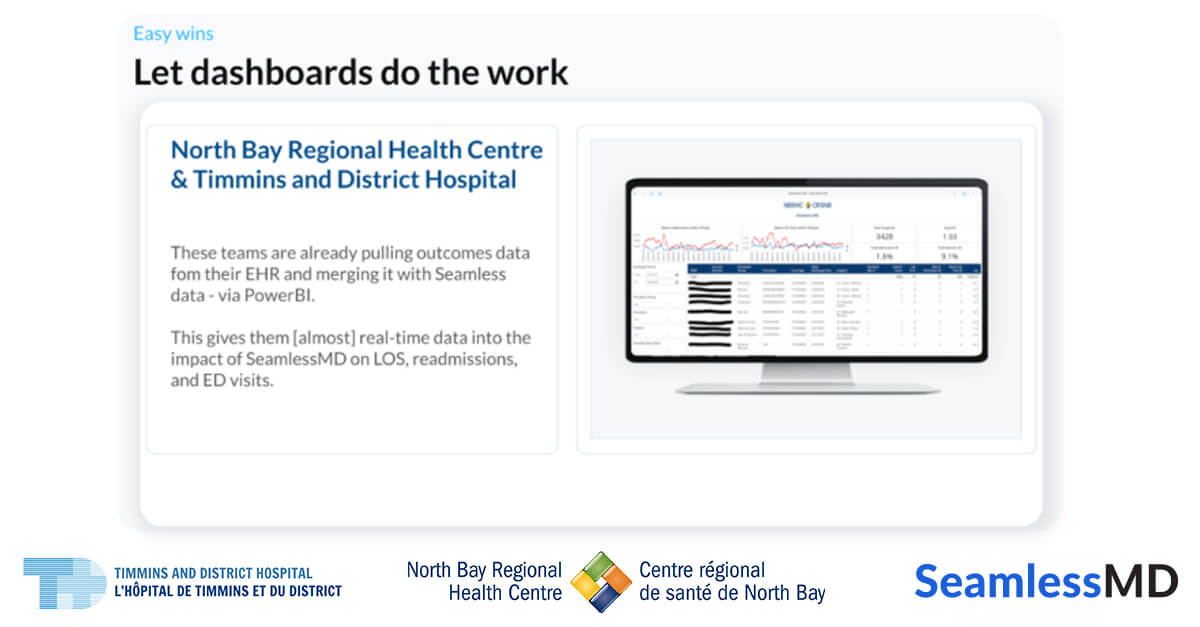
Deciphering which data is available, in what format, and how to leverage it in a meaningful way is often challenging, even more so when looking at data as ERAS programs expand across multiple pathways. ERAS leaders that manage data across pathways suggest that having standardized dashboards, and monitoring them consistently, ensures that any trends or anomalies can be identified and acted upon.
Dashboards and databases
For instance, Vicki explains at Novant Health they have “a database and a dashboard that is looked at frequently. A lot of it used to just be very much manually extracted data. We've moved into a lot of automation now. Still some manual extraction, but a lot of automation, which has helped. I love our database. I love that we collect as much data as we do because it gives us so much information and really helps us to evaluate and mold our program.”
And when it comes to noticing any variability for specific metrics being measured, it is acted upon “right away because we're looking at our data constantly and it's pretty real-time. Even as it's being entered...I look at it every single day. We report it every month, but even if it's small - half a day change or 10% difference or whatever - it's a discussion of - for instance, compliance - saying, ‘did we hire a bunch of new nurses? We're in between education and do we need to get educators over there now? What's been going on?’” shares Vicki.
Manual data collection
Gina McConnell, ERAS Cardiac Nurse Coordinator at WakeMed, echoes the value dashboards can bring to data collection and monitoring as the ERAS pathways expand. But she emphasizes that the key is to ensure that data is collected, regardless of how big or small your ERAS pathway may be and what tools you have at your disposal.
She shares that “when we first started ERAS, we started with cardiac - so we had the STS guideline and we had our STS data … Then we manually extracted for a year and so we didn't have the luxury of intervening day to day or week to week. Now we've matured and we have a dashboard that gives us almost live data. That's the luxury - now we can intervene. If you're starting a program and you just have Excel, that's okay. You at least have data that you can monitor and as you evolve and mature, you'll have data that you can monitor daily instead of quarterly. You're retrospectively going back and fixing things when you have an Excel spreadsheet or paper as we say. But maturing to these dashboards now, it's taken us several years to get to these dashboards. It's been a lot of work and we've grown, but we started out just having to use what we had and be able to intervene as we could.”
Even with dashboards, however, manual audits might still be necessary as required, according to Charlette. She shares that at Baylor, they “used to manually abstract charts and then we would put it into Excel. Now we have based our populations off of medical coding. So we have gotten rid of all manual audits. The caveat is if you see something that's trending in the wrong direction, sometimes you have to dig deeper to figure out, ‘Well, why are we trending that way?’ So then you may need to do a snapshot of manual data auditing. At the end of the day, “we want our nurses, our surgeons, our anesthesia providers taking care of the patients, not focusing on abstracting data. So, we try to get rid of that as much as we possibly can.”
In Summary
An ERAS program’s success relies heavily on standardized implementation of protocols, measuring the right data points and continuously optimizing the program by learning from those outcomes. Having comprehensive data also enables care teams to make a case for scaling ERAS - as healthcare providers and patients become accustomed to seeing improved clinical outcomes, they become motivated to use ERAS protocols and there continues to be studies published on the effectiveness and economic impact of ERAS programs.
For insights on pathway specific outcomes to measure and protocols to follow, watch the on-demand webinar with Gina, Vicki, and Charlette, where they also dive into surgery-specific processes around using immuno nutritional drink, the impact of ERAS on SSI rates, carb loading, and performing blocks with anesthesia.
If you’d like to learn how Digital Care Journeys are being used by leading health systems to automate ERAS pathways, measure patient compliance, automate the collection of PROs, and improve outcomes, watch this session with Dr. Joshua Liu, book a demo here, or get in touch with us at info@seamless.md.




.png)
